

A Face to a Name
On PMOS, the rename, and a conversation long overdue


Welcome to the Michelle Seguin MD newsletter! I’m Dr. Michelle, and I’m so glad you’re here. This week, a long-overdue recognition in women's health: what PMOS is, why the rename matters, how I approach care, and something personal I've been meaning to share.

Hello friends,
Last week, a paper published in The Lancet serves as the inspiration for this week’s letter. A global consortium of more than 50 academic, clinical, and patient organizations, drawing on input from over 14,000 women living with the condition, formally recognized that polycystic ovary syndrome, PCOS, has been misnamed for decades. The new name, polyendocrine metabolic ovarian syndrome, or PMOS, reflects what this condition actually is: a whole-body hormonal and metabolic syndrome.
The authors were clear about why the old name wasn’t just imprecise, but also potentially harmful. It reflected only one organ while failing to capture a multi-system disorder. It delayed diagnosis, hindered communication between patients and clinicians, reinforced stigma, and limited the research questions that got asked. My hope is that this letter shines light on an often misunderstood condition, and puts a face to a name.
With gratitude,
Dr. Michelle

What PMOS Actually Is
"PCOS encompasses diverse endocrine, metabolic, reproductive, psychological, and dermatological features. The current name reflects only one organ and fails to capture the disorder's multisystem nature." — Teede et al., The Lancet, May 2026
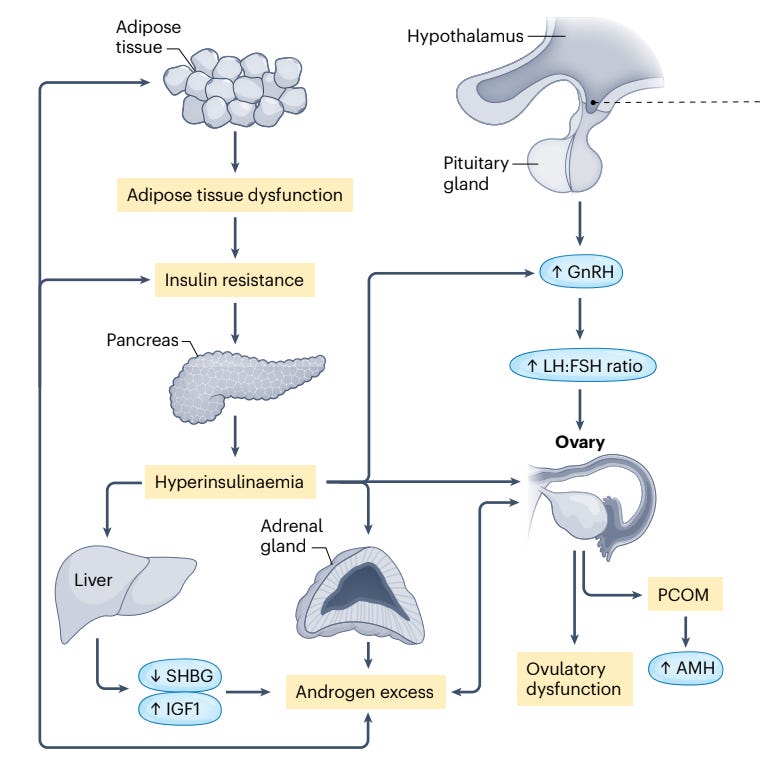
PMOS involves three overlapping processes that reinforce one another and, when left unaddressed, compound over time:
Insulin resistance - The body's cells become less responsive to insulin, prompting the pancreas to produce more of it. Elevated insulin then signals the ovaries to produce excess androgens, including testosterone — the central metabolic thread running through the condition, with implications that extend well beyond reproductive health.
Androgen excess - Elevated androgens, particularly testosterone and DHEA-S, drive many of the most visible and often distressing symptoms: acne that doesn't respond to typical treatments, excess hair growth on the face and body, and hair thinning at the scalp. These are not cosmetic inconveniences. For many women they carry significant emotional distress, affecting self-image and quality of life in ways that clinical encounters often underestimate. Excess androgens also interfere with normal follicle development in the ovaries, disrupting ovulation and leading to the irregular or absent cycles.
HPA axis dysregulation - The hypothalamic-pituitary-adrenal axis governs the body's stress response, and in PMOS it is frequently dysregulated. Chronic stress amplifies cortisol output, which further stimulates androgen production and worsens insulin sensitivity. Sleep deprivation, sustained psychological stress, and a life without adequate recovery are not merely generally hard on the body; for women with PMOS, they are mechanistically significant in ways that show up on labs and symptoms.
How Is PMOS Diagnosed?
Diagnosis is currently made using the Rotterdam Criteria, which require two of the following three features:
1. Irregular or absent menstrual cycles: Cycles that are consistently shorter than 21 days or longer than 35 days, absent periods, or fewer than 8 cycles per year.
2. Clinical or biochemical signs of androgen excess: This includes symptoms such as acne, excess facial or body hair (hirsutism), or scalp hair thinning, as well as elevated testosterone or DHEA-S on laboratory testing.
3. Polycystic ovarian morphology on ultrasound, or elevated AMH: 12 or more follicles measuring 2–9mm in one or both ovaries, increased ovarian volume, or an elevated anti-Müllerian hormone (AMH) level on blood testing. AMH was added to adult diagnostic criteria in the 2023 international guidelines as a more accessible and reproducible alternative to ultrasound.
Important to note: other conditions that cause irregular cycles or androgen excess — including thyroid disease, elevated prolactin, and congenital adrenal hyperplasia — must be ruled out before a diagnosis is confirmed in certain cases.
One of the most important things I tell patients is that no two cases of PMOS are the same. It is a syndrome that exists on a spectrum, and how it shows up in one woman's body may look quite different from how it shows up in another's.
Common symptoms include:
Irregular, infrequent, or absent periods
Acne, particularly along the jawline and chin
Excess hair growth on the face, chest, or abdomen (hirsutism)
Hair thinning or loss at the scalp
Difficulty losing weight or unexplained weight gain
Fatigue and low energy
Mood changes, anxiety, or depression
Skin tags or darkening of the skin in skin folds (acanthosis nigricans)
Difficulty conceiving
Severity varies widely, and many women recognize only a few of these. That is still enough to warrant a conversation with your provider.
One thing that makes PMOS particularly difficult to recognize is that it doesn’t present the same way in every woman. Some have irregular cycles and visible cysts on ultrasound. Others, like many of my patients, have entirely regular periods but carry the metabolic and androgenic features of the condition without any of the reproductive signals that typically prompt investigation. The pattern of elevated androgens with regular cycles is among the most commonly missed, because nothing on the surface looks wrong. This is one reason the diagnostic gap is so large — estimates suggest up to 70% of cases remain undiagnosed.
The Full Risk Picture
Another important aspect of the new name is that it finally brings into view the risks the old framework obscured. PMOS is not primarily a condition of fertility, though it profoundly affects fertility for many women. Its reach extends across multiple organ systems and across a woman's full lifespan.
Metabolic and cardiovascular risk - Women with PMOS have significantly higher rates of insulin resistance, type 2 diabetes, dyslipidemia, and hypertension. The Lancet consensus cites a 68% increased odds of cardiovascular disease, including a more than doubled risk of myocardial infarction. This risk is real and often underappreciated, particularly in younger women whose care has often been organized around reproductive concerns rather than metabolic monitoring.
Fertility and reproductive health - Ovulatory dysfunction is a defining feature of PMOS, and for women trying to conceive, it is often the first moment the condition surfaces in clinical care. Irregular or absent ovulation makes conception more difficult, and pregnancy complications including gestational diabetes are more common. Many women with PMOS do conceive, with or without intervention, and a diagnosis is not a sentence. It is, however, a reason for thoughtful, proactive care.
Mental health - Depression, anxiety, and eating disorders occur at substantially higher rates in women with PMOS, and the relationship is bidirectional — the hormonal and metabolic features of the condition contribute to mood dysregulation, and psychological stress in turn worsens the metabolic picture. A growing body of research also suggests that women with PMOS report higher rates of adverse childhood experiences (ACEs), which may contribute to HPA axis dysregulation in ways that amplify the condition's hormonal burden. Asking about early adversity (i.e. screening for ACEs) is part of caring well for someone with PMOS.
Endometrial cancer - Without regular ovulation, the uterine lining is exposed to ongoing estrogen without the progesterone that would normally follow, increasing risk for endometrial hyperplasia and cancer. This risk is manageable with appropriate monitoring and hormonal support when indicated.
Menopause and beyond - Women with PMOS tend to reach menopause later than their peers, by approximately two to four years, likely due to higher AMH levels and greater follicle reserves. As estrogen declines during the perimenopausal transition, the relative androgenicity can intensify, and insulin resistance, inflammation, and dyslipidemia often worsen rather than resolve. Women who managed PMOS well during their reproductive years sometimes find symptoms re-emerging through perimenopause. Interestingly, a recent study published last month suggests that vasomotor symptoms, such as hot flashes, may be less prominent in women with PMOS, possibly due to the buffering effect of persistent androgens though the research is still evolving.
How I Approach Care for Women With PMOS
When a patient comes to me with a PMOS diagnosis, or with a constellation of symptoms pointing toward it, my first instinct is to zoom out. The conventional approach often narrows quickly to the presenting symptom — irregular cycles, acne, a fertility concern — and addresses each in relative isolation. What I’ve found more useful is to begin with the full metabolic picture and work outward from there.
Care is always personalized. Advanced testing helps build an accurate picture that guides individualized recommendations, and typically includes:
Fasting insulin, fasting glucose, hemoglobin AIC to assess insulin resistance, glycemic control
Androgen panel including total testosterone, DHEA-S, and in some cases further hormone testing with AMH, prolactin, AM cortisol
Inflammatory markers including hs-CRP
Lipid panel, and in some cases advanced markers including LPa, ApoB, lipid fractionation, omega-3 / omega-6 levels
Full thyroid panel
Hepatic (liver) function panel
Micronutrient panel including vitamin D, ferritin, zinc, magnesium
From there, treatment is built around each woman’s specific pattern, priorities, and life stage through team-based physician / registered dietitian (RD) care. That may include targeted supplementation (myo-inositol, NAC, magnesium, and vitamin D all have meaningful evidence in PMOS) alongside dietary and lifestyle interventions, continuous glucose monitoring (CGM) trials if appropriate, and pharmaceutical support when indicated. The goal is personalization, not a generic protocol.
Food as a primary lever - Anti-inflammatory, low-glycemic eating patterns that emphasize vegetables, legumes, whole grains, healthy fats, and quality proteins consistently show improvements in insulin sensitivity and androgen levels. The Mediterranean dietary pattern has the strongest evidence base, but the underlying principles translate across many food traditions. Dietary diversity matters here, too, as a wide variety of plants supports the gut microbial diversity that increasingly appears relevant to androgen metabolism and hormonal signaling. An emerging area of research points to gut dysbiosis as a meaningful thread in PMOS pathophysiology, with altered bile acid metabolism and reduced microbial diversity both documented in women with the condition. More fiber, more variety, more fermented foods — this is where the science and the garden meet!
In practice, I try to move the conversation away from restriction and toward abundance. At Root, we use a simple plating method designed with blood sugar balance in mind — the PFC method, which ensures each meal includes a quality protein, a healthy fat, and a fiber-rich carbohydrate alongside plenty of non-starchy vegetables. It's a flexible framework, not a rigid plan, and it translates across cooking traditions and flavor preferences. You can read more about it here and see it applied to PCOS-specific meals.
Movement - Both aerobic exercise and resistance training show meaningful benefits for insulin sensitivity and androgen levels in women with PMOS. I encourage patients to choose movement they genuinely enjoy and will sustain, and to let variety and seasonality guide them — the body thrives when it's asked to do different things across time, and outdoor movement carries particular value for a condition driven in part by HPA axis dysregulation. I explored the research behind movement variety in a recent letter if you'd like to read more.
Sleep and stress - Sleep deprivation worsens insulin sensitivity within days. Chronic stress sustains the cortisol output that drives androgen production. These levers matter more than we may realize. In practice, I discuss stress reduction practices including breath work, meditation, journaling, and yoga as starting points, and for some patients, more intensive nervous system and limbic retraining support.
The mental health conversation - Given the elevated rates of depression, anxiety, and disordered eating in women with PMOS, I make space for this conversation explicitly rather than waiting for it to surface on its own. How a patient feels in her body matters as much as what her labs show, and sometimes it matters more. For women with trauma histories, I think about coping patterns as part of the clinical picture and consider referral to behavioral support as part of integrated care.
Throughout all of this, I try to hold the condition with patience and generosity — toward my patients and toward the complexity of what we're working with. This is not a condition that resolves with a six-week protocol. It is a condition that requires tending, across years and seasons, with the goal of stability and a life well-lived.
A Personal Note
PMOS affects an estimated 1 in 8 women worldwide. I am one of them.
My own path toward food as medicine, lifestyle medicine, and functional medicine, was shaped, more than I fully understood at the time, by my own experience of living with PMOS. It is not uncommon for physicians (and other health professionals) to find their way toward integrative approaches through a health challenge of their own (or a loved one).
The garden and the kitchen have been central to how I’ve tended life with it. So has sleep, and movement, and the particular type of restoration that comes from time along the Lake Superior shoreline, or in the woods and garden on our property. I have had seasons when the conditions of my life supported this well, and seasons when they didn’t, and the difference showed up in my body in ways I now understand far more clearly than I did when I was inside them. I am still learning alongside you.
There is more to say, and I’ll write more in the future, because the full story is longer than a closing paragraph can hold. But I wanted to give it voice here, alongside news that finally names the condition for what it is. Physicians are people, too. Many of us came to this work carrying something of our own. The more willing we are to say so, the more we contribute to reducing the stigma that has surrounded this condition for too long.
If you recognize yourself or someone you care about in any of what I’ve written here, I’d love to hear from you. You can reply to this email directly or respond in the comments below.
In Closing
Writing this letter has meant something special to me, and I'm grateful for the space this community creates to share not just the science, but the story behind it. If PMOS is a topic you'd like me to return to, whether the research continues to evolve, the personal story deepens, or you simply have questions you'd like explored, I'd love to hear that. These letters are always a conversation.
With love and care,
Dr. Michelle
P.S. If this note resonates, please give it a like or share it with a friend. When they subscribe, you’ll earn rewards as a thank you.
Work With Me
If you’re curious about working together clinically, I see patients through Root Functional Medicine, a telemedicine practice specializing in personalized lifestyle and functional medicine. I’m currently licensed in Michigan and 28 additional states, so there’s a good chance I can see you wherever you are. You can learn more and inquire about availability here.

A reminder that this week, on May 20th 4pm EST/1pm PST, I am joining Beth Bollinger , Anja Lee Hall, and the Blood Sugar Method community for my first seasonal workshop collaboration. We will be discussing how seasonal eating, dietary diversity, and even a small container garden can support metabolic health and reduce inflammation over time.
Registration is open to all if you would like to join us!
Here are my most recent Substack sharings:
Michelle, this is such a fantastic breakdown of what PMOS is, why the name had to change (finally!), and how to manage it. As an ob/gyn, I am acutely aware of the impact this syndrome has had on so many people. Raising awareness about its implications in heart and brain health risk is much needed. Thank you!
Thank you Michelle for sharing this. I have a handful of clients and a lot of books. Looks like it's time to go back to the drawing board.